Sep
8
2023
Unwinding as an ideomotor action
Barret Dorko (2003) suggested that fascial unwinding can be explained as ideomotor movement (ideomotion). He postulated that cranial techniques founded by Sutherland and palpated inherent tissue movement fall into this category. As stated by Ward (2002):
“Inherent tissue motions are palpably evident, asymmetrically patterned, neuroreflexive activities in the soft tissues. They constantly move, often at variable rates. Palpation that focuses on these motions should readily identify patterns of shifting asymmetric tightness and looseness.”
Ideomotor action or ideomotion is “influence of suggestion in modifying and directing muscular movement, independently of volition”, a definition given by psychologist/physiologist William Carpenter in 1852.
Carpenter used ideomotor action as an explanation for various phenomena that were being credited to new physical forces, spiritual intervention, or other supernatural causes (Hyman, 1999). Later, William James in 1890 proposed a wider meaning that ideomotor activity is the basic process underlying all volitional behavior:
Ideomotor action also pertains to body movements that can arise in observers watching other people perform certain actions (Knuf et al., 2001). Muscles can be involuntarily activated by thoughts. Involuntary muscle movement can manifest in various ways, for example asking a subject to think of an activity is enough to set the muscles required for that activity into action (Spitz, 1997).
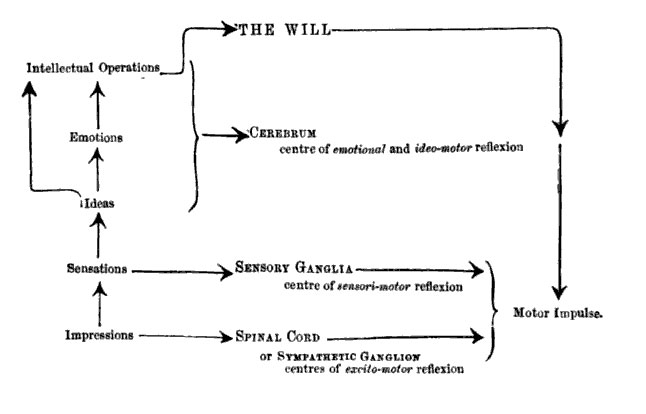
Carpenter (1860) characterized ideomotor action as a third law of reflex. Apparently at that time reflex movements are partitioned into two kinds: excito-motor (such as breathing and swallowing), and sensory-motor (such as surprise-reactions to a loud noise). Carpenter imagined the processing of stimuli and the generation of action as a bottom-up path of information processing. In the normal course of processing external impressions evoke sensations, ideas, emotions, and intellectual processes that determine the will. Then the will initiates the actions to be executed. But if the path of processing is interrupted at any point, Carpenter suggested that a reflex action occurs (Stock and Stock, 2004).
On the lower levels there are excito-motor reflexes, which are controlled by the spinal cord. On the next highest level of processing sensory-motor reflexes set in, controlled by the sensory ganglia. Finally, the ideo-motor reflexes occur, when the will, as the highest controller, is turned off in some way. In this case ideas and emotions gain direct access to action execution through reflexes (Figure 1, Carpenter, 1860).
Dorko (2003) hypothesized the mechanism of unwinding as follows: “Muscular pain can arise from mechanical deformation of various tissues. If the movement required for reducing that injury is not permitted because of cultural norms, the body would respond with an array of isometric contraction of muscular activity.”
Dorko further hypothesized that this muscle activity is commonly misinterpreted as a lack of appropriate relaxation, and subjected to various forms of stretching, manipulation or exercise. Unwinding allows full expression of the muscles and encourages completing the motor response for which the contraction was activated. The touch by the therapist is gentle and non-coercive, with a goal to make the client aware of internal motor activity and then get out of the way of that movement.
This seems to be in accordance with the Rosen method (Rosen and Brenner, 2003) which believes that our bodies and characters are shaped by the social factors, developing habitual patterns of holding and restriction in order to be socially appropriate. Our muscles were tightened to inhibit the expression of emotions and physical motions of defense. These inhibited emotions and motions are stored in the body limiting our freedom of expression and movement.
McCarthy et al. (2007) suggested that the resolution of muscular pain is dependent on an appropriate motor response, and such a response should proceed as the result of instinctive, in-built mechanisms. Ideomotor movements constitute the prevailing expression of instinctive movement response. They hypothesized that the corrective ideomotor movement expression may lead to improvements in pain intensity and disability in symptomatic clients whose instinctive responses have been suppressed.
Sep
8
2023
Beware! Books from Alphascript and Betascript
Since last year, a large number of books are available from the web, including ebay and Amazon.com. Hundreds of thousands of books are published under Alphascipt, Betascript,and Fastbook Publishing. These are scam companies making money by publishing books using Wikipedia as materials. The whole book is made up of wikipedia articles, which are free. They grabbed the articles from a free source and making money out of that. The cover of the book says “High Quality Content by Wikipedia Articles”.
These publishing companies are just examples of thousands of the so called “Print on Demand” books. Meaning that they list the title, and they will only print the book when it is being ordered. Even big companies like Elsevier are now using this Print on Demand method, they don;t need to stock their books anymore.
But what’s worrying are the scam companies that me money out of selling books where the contents are from free materials such as Wikipedia. It is on sale in many of the famous online book sellers including Amazon.com.
Amazon.com has more than 100,000 titles of the scam books by Alphascript, more than 600,000 titles under Betascript, and more than 1000 titles under Fastbook. And each book is sold quite expensive, more than $50 per book!
The Alphascript books (more than 100,000) are all written by FREDERIC P. VANDOME, AGNES F. MCBREWSTER, JOHN MILLER
Betascript books (more than 600,000) are all written by LAMBERT M. TENNOE, MARIAM T. HENSSONOW, SUSAN F. SURHONE
These authors must be so productive that they can write that many books in just 1 year!
So beware! Don’t just buy any thitle without reading the review and exact content.
Update:
We got a letter from a representative from Alphascript requesting us not to mention the word SCAM http://www.massage-research.com/blog/?p=1215 This book by Betascript tells it all:
Sep
7
2023
Regular stretch does not increase muscle extensibility
Scand J Med Sci Sports. 2010 Feb;20(1):136-44. Epub 2009 May 22.
Regular stretch does not increase muscle extensibility: a randomized controlled trial.
Ben M, Harvey LA.
The purpose of this randomized controlled trial was to determine whether regular stretch increases hamstring muscle extensibility.
Sixty healthy individuals were randomly allocated to an experimental or a control group. The experimental group attended supervised stretch sessions where they stretched the hamstring muscles of a randomly allocated leg for 30 min five times a week for 6 weeks. The control group did not attend any stretch sessions during this period. No participants withdrew from the study.
A purpose built device was used to measure passive hip flexion during a straight leg-raise manoeuvre with the application of a standardized and non-standardized stretch torque.
The stretch intervention did not increase passive hip flexion when measured with a standardized stretch torque [mean treatment effect=-1 degrees; 95% confidence interval (CI)=-3 to 2 degrees]. It did, however, increase passive hip flexion when measured without a standardized stretch torque (mean treatment effect=10 degrees, 95% CI=6-14 degrees).
Six weeks of sustained 30-min daily stretch does not increase the extensibility of the hamstring muscle of healthy individuals. It does, however, improve stretch tolerance leading to increased joint range of motion without any actual improvements in muscle extensibility.
Sep
7
2023
Massage impairs postexercise muscle blood flow and “lactic Acid” removal
Wiltshire, E.V., Poitras, V., Pak, M., Hong, T., Rayner, J., Tschakovsky, M.E. 2010
Medicine and Science in Sports and Exercise 42 (6), pp. 1062-1071
PURPOSE: This study tested the hypothesis that one of the ways sports massage aids muscle recovery from exercise is by increasing muscle blood flow to improve “lactic acid” removal.
METHODS: Twelve subjects performed 2 min of strenuous isometric handgrip (IHG) exercise at 40% maximum voluntary contraction to elevate forearm muscle lactic acid. Forearm blood flow (FBF; Doppler and Echo ultrasound of the brachial artery) and deep venous forearm blood lactate and H concentration ([La-], [H+]) were measured every minute for 10 min post-IHG under three conditions: passive (passive rest), active (rhythmic exercise at 10% maximum voluntary contraction), and massage (effleurage and pétrissage). Arterialized [La-] and [H+] from a superficial heated hand vein was measured at baseline.
RESULTS: Data are presented as mean ± SE. Venoarterial [La -] difference ([La-]v-a) at 30 s of post-IHG was the same across conditions (passive = 6.1 ± 0.6 mmol•L -1, active = 5.7 ± 0.6 mmol•L-1, massage = 5.5 ± 0.6 mmol•L-1, NS), whereas FBF was greater in passive (766 ± 101 mL•min-1) versus active (614 ± 62 mL•min-1, P = 0.003) versus massage (540 ± 60 mL•min, P < 0.0001).
Total FBF area under the curve (AUC) for 10 min after handgrip was significantly higher in passive versus massage (4203 ± 531 vs 3178 ± 304 mL, P = 0.024) but not versus active (3584 ± 284 mL, P = 0.217). La- efflux (FBF × [La-] v-a) AUC mirrored FBF AUC (passive = 20.5 ± 2.8 mmol vs massage = 14.7 ± 1.6 mmol, P = 0.03, vs active = 15.4 ± 1.9 mmol, P = 0.064). H+ efflux (FBF × [H+]v-a) was greater in passive versus massage at 30 s (2.2 ± 0.4e-5 vs 1.3 ± 0.2e-5 mmol, P < 0.001) and 1.5 min (1.0 ± 0.2e-5 vs 0.6 ± 0.09e-5 mmol, P = 0.003) after IHG.
CONCLUSIONS: Massage impairs La and H+ removal from muscle after strenuous exercise by mechanically impeding blood flow.
Sep
7
2023
Massaging Muscles Facilitates Recovery After Exercise
Olympic swimmer Michael Phelps got a massage twice a day in Beijing. His teammate, Dara Torres, had two massage therapists on stand-by.
Researchers testing the long-held theory that therapeutic massage can speed recovery after a sports injury have found early scientific evidence of the healing effects of massage.The scientists have determined that immediate cyclic compression of muscles after intense exercise reduced swelling and muscle damage in a study using animals.

Though they say it’s too soon to apply the results directly to humans in a clinical environment, the researchers consider the findings a strong start toward scientific confirmation of massage’s benefits to athletes after intense eccentric exercise, when muscles contract and lengthen at the same time.
“There is potential that this continuing research will have huge clinical implications,” said Thomas Best, a professor of family medicine at Ohio State University and senior author of the study. “If we can define the mechanism for recovery, the translation of these findings to the clinic will dictate how much massage is needed, for how long, and when it should be performed after exercise.”
Anecdotal evidence suggests massage offers many health benefits, but actual testing of its effects at the cellular level is more difficult than one might think. In this study with rabbits, the researchers used one mechanical device to mimic movements associated with a specific kind of exercise, and a second device to follow the exercise with a simulated consistent massaging motion on the affected muscles. They compared these animals to other animals that performed the exercise movements but did not receive simulated massage. All animals were sedated during the experiments.
“We tried to mimic Swedish massage because anecdotally, it’s the most popular technique used by athletes,” said Best, who is also co-medical director of the OSU Sports Medicine Center and a team physician for the Department of Athletics. “A review of the research in this area shows that despite the existing anecdotal evidence – we know athletes use massage all the time – researchers don’t know the mechanism of how massage improves recovery after exercise and injury.”
Swedish massage combines long strokes, kneading and friction techniques on muscles and various movements of joints, according to the American Massage Therapy Association.
After the experimental exercise and massage were performed in the study, the researchers compared the muscle tissues of all of the animals, finding that the muscles in animals receiving simulated massage had improved function, less swelling and fewer signs of inflammation than did muscles in the animals that received no massage treatment after exercise.
The research is published in a recent issue of the journal Medicine & Science in Sports & Exercise.
The research focused on eccentric exercise, which creates a motion similar to the way in which quadriceps in human thighs are exercised during a downhill run. In the study, the scientists focused on the tibialis anterior muscle, located on the front of the shin in humans. The simulated exercise involved continuous flexing and pointing of the toes to exert the muscle during seven sets of 10 cycles, with two minutes of rest between each set.
“It’s hard to describe exactly how the exercise intensity would be matched in a human, but this was considered a significant amount of exercise that would likely cause muscle soreness and possible damage,” Best said.
Immediately following the exercise, the affected muscle was subjected to 30 minutes of simulated massage, called compressive loading. The researchers used mathematical equations to determine the appropriate amount of force to apply to the animal muscle, which was intended to match the force Swedish massage typically places on a patient’s spine. The device used to simulate the stroking motion for the research was designed by Yi Zhao, assistant professor of biomedical engineering at Ohio State and a co-author of the study.
“We know biological tissues are sensitive to the magnitude of frequency, duration and load, so we controlled the force, frequency and time spent on massage,” Best said.
The exercise-massage cycle was repeated for four days, after which the animals’ muscle strength and tissue were examined.
The massaged muscles recovered an estimated 60 percent of the strength after the four-day trial, compared to restoration of about 14 percent of strength in muscles that were exercised and then rested.
Similarly, the massaged muscles had fewer damaged muscle fibers and virtually no sign of white blood cells, the presence of which would indicate that the body was working to repair muscle damage, when compared with the rested muscles. The massaged muscles weighed about 8 percent less than the rested muscles, suggesting that the massage helped prevent swelling, Best said.
“One fundamental question is how much of a role does inflammation play in repair to a muscle? Are we preventing inflammation and therefore improving recovery? We haven’t proven that yet,” Best said.
He is collaborating with a variety of experts across the university to continue this line of research, and hopes to cooperate with Ohio State’s Center for Integrative Medicine on future clinic-based work.
“Our goal is to use this model to understand the biological mechanisms of massage as a guide to preclinical trials to test the effects of massage on muscle recovery after exercise,” he said. “A trial in humans could look at optimal indications for massage.
“Ultimately, we could also find out how massage helps not just exercise-induced muscle injury, but swelling and pain associated with other medical conditions, as well.”
Ohio State University (2008, August 12). Massaging Muscles Facilitates Recovery After Exercise. ScienceDaily.
Sep
7
2023
Intensive exercise prevented shortening of telomeres, a protective effect against aging of the cardiovascular system, according to research reported in Circulation: Journal of the American Heart Association.
Researchers measured the length of telomeres — the DNA that bookends the chromosomes and protects the ends from damage — in blood samples from two groups of professional athletes and two groups who were healthy nonsmokers, but not regular exercisers.
The telomere shortening mechanism limits cells to a fixed number of divisions and can be regarded as a “biological clock.” Gradual shortening of telomeres through cell divisions leads to aging on the cellular level and may limit lifetimes. When the telomeres become critically short the cell undergoes death. The 2009 Nobel Prize in Physiology or Medicine was awarded to researchers who discovered the nature of telomeres and how chromosomes are protected by telomeres and the enzyme telomerase.
“The most significant finding of this study is that physical exercise of the professional athletes leads to activation of the important enzyme telomerase and stabilizes the telomere,” said Ulrich Laufs, M.D., the study’s lead author and professor of clinical and experimental medicine in the department of internal medicine at Saarland University in Homburg, Germany.
“This is direct evidence of an anti-aging effect of physical exercise. Physical exercise could prevent the aging of the cardiovascular system, reflecting this molecular principle.”
Essentially, the longer telomere of athletes is an efficient telomere. The body’s cells are constantly growing and dividing and eventually dying off, a process controlled by the chromosomes within each cell. These chromosomal “end caps” — which have been likened to the tips of shoelaces, preventing them from fraying — become shorter with each cell division, and when they’re gone, the cell dies. Short telomeres limit the number of cell divisions, Laufs said. In addition, the animal studies of Laufs and colleagues show that the regulation of telomere stabilizing proteins by exercise exerts important cellular functions beyond the regulation of telomere length itself by protecting from cellular deterioration and programmed cell death.
In the clinical study, researchers analyzed 32 professional runners, average age 20, from the German National Team of Track and Field. Their average running distance was about 73 kilometers (km), a little over 45 miles, per week.
Researchers compared the young professional athletes with middle-aged athletes with a history of continuous endurance exercise since their youth. Their average age was 51 and their average distance was about 80 km, or almost 50 miles, per week.
The two groups were evaluated against untrained athletes who were healthy nonsmokers, but who did not exercise regularly. They were matched for age with the professional athletes.
The fitness level of the athletes was superior to the untrained individuals. The athletes had a slower resting heart rate, lower blood pressure and body mass index, and a more favorable cholesterol profile, researchers said.
Long-term exercise training activates telomerase and reduces telomere shortening in human leukocytes. The age-dependent telomere loss was lower in the master athletes who had performed endurance exercising for several decades.
“Our data improves the molecular understanding of the protective effects of exercise on the vessel wall and underlines the potency of physical training in reducing the impact of age-related disease,” Laufs said.
Sep
7
2023
The immediate effects of traditional Thai massage on heart rate variability and stress-related parameters in patients with back pain associated with myofascial trigger points
Vitsarut Buttagat B.Sc., M.Sc., PhD candidate, Wichai Eungpinichpong B.Sc., M.Sc., PhD, Uraiwon Chatchawan B.Sc., M.PH., PhD and Samerduen Kharmwan MD
Journal of Bodywork and Movement Therapies
Summary
The purpose of this study was to investigate the immediate effects of traditional Thai massage (TTM) on stress-related parameters including heart rate variability (HRV), anxiety, muscle tension, pain intensity, pressure pain threshold, and body flexibility in patients with back pain associated with myofascial trigger points. Thirty-six patients were randomly allocated to receive a 30-min session of either TTM or control (rest on bed) for one session. Results indicated that TTM was associated with significant increases in HRV (increased total power frequency (TPF) and high frequency (HF)), pressure pain threshold (PPT) and body flexibility (p < 0.05) and significant decreases in self-reported pain intensity, anxiety and muscle tension (p < 0.001). For all outcomes, similar changes were not observed in the control group. The adjusted post-test mean values for TPF, HF, PPT and body flexibility were significantly higher in the TTM group when compared with the control group (p < 0.01) and the values for pain intensity, anxiety and muscle tension were significantly lower. We conclude that TTM can increase HRV and improve stress-related parameters in this patient population.
Sep
7
2023
Disease-a-Month
Volume 55, Issue 3, March 2009, Pages 121-192  doi:10.1016/j.disamonth.2008.12.002 Alternative and Complementary Medicine for Preventing and Treating Cardiovascular Disease
doi:10.1016/j.disamonth.2008.12.002 Alternative and Complementary Medicine for Preventing and Treating Cardiovascular Disease
A review of Alternative and Complementary Medicine for Preventing and Treating Cardiovascular Disease was recently published in Disease-a-month journal.
The authors concluded that: Alternative medicine represents those healing traditions that in the recent past were not part of standard allopathic medical training. However, more and more individuals are seeking CAM practitioners and remedies for part of their health care needs. Although most CAM therapies are relatively innocuous and often improve patient well-being most likely through a placebo effect, some involve the use of pharmacologically active substances (eg, herbal medicine, megavitamin therapy, and some folk remedies) that could complicate existing medical therapy or even cause harm.
Physicians must be aware of CAM practices so that they can best counsel their patients in an atmosphere of open communication. Rather than dismissing a patient’s highly motivated intentions toward health-conscious behaviors, it behooves the physician to understand the range of CAM treatments and when they might be safely integrated with conventional medicine.
Despite the lack of scientific rigor in previous studies of CAM therapies, the NCCAM, a part of the NIH, is now actively coordinating clinical trials, advancing scientific research, and training researchers to study CAM. Ultimately it will be the fusion of the best medical practices from those which are rigorously studied in clinical trials that will provide the most favorable clinical outcomes in medicine.
In addition, physicians must remember that many of our current drugs came out of herbal medicine practice (eg, digitalis, aspirin, lovastatin, reserpine), and homeopathy (nitroglycerin). Much of our bedside approach to sick patients was adopted and modified from ancient and deeply rooted cultures (eg, Ayurveda). We have the responsibility as medical professionals to preserve and protect the physical, psychological, and spiritual “heart” of our patients. Achieving a “placebo effect,” while doing “no harm,” is a benefit clinicians should not ignore.
Massage Therapy
Massage therapy has been available for centuries; however, the idea of therapeutic or healing touch was strongly promoted in the 1970s. Although the theory of “energy transfer” to patients with cardiovascular disease has been postulated, there is no scientific substantiation of this concept. There is more evidence of a potential anti-anxiety effect, which bears further scrutiny. A study by Song et al. analyzed electroencephalograms and electrocardiograms in 22 subjects who focused attention on their heartbeats with and without kinesthetic (touch) biofeedback. Heart-focused attention and awareness of creative pulsations revealed increased electroenceph-alographic activities synchronized with the electrocardiogram, possibly reflecting increased baroreceptor and somatosensory feedback. This suggests a homeostatic self-regulation between the brain and the target organ, which may underlie the self-healing mechanisms apparent in mind-body medicine.
Tiller et al. demonstrated that patients trained in heart-focused stress reduction techniques shifted attention away from stress and directly influenced the parasympathetic feedback loop.299 These and other studies on the physiology of self-attention provide a crossover reference to the effects demonstrated with therapeutic touch. Heidt studied 90 patients who were hospitalized in a cardiovascular unit, comparing the effects of therapeutic touch, casual touch, or no touch with all patients receiving a 5-minute intervention. Pre- and postinterventional anxiety scores showed a significantly greater reduction in post touch anxiety among the patients receiving therapeutic touch. An extensive review of the literature concludes that there is evidence to support the practice of therapeutic touch for the reduction of both pain and anxiety. Nine of 11 studies analyzed showed statistically significant benefits from this treatment.
Massage therapy has a long history of use for musculoskeletal and orthopedic complaints with a variety of positive responses reported. There have been relatively few studies in regard to the treatment of cardiovascular patients and any long-term benefit. One study by Olney found regular therapeutic massage to be helpful in lowering blood pressure in hypertensive patients. McNamara et al. studied back massage before diagnostic cardiac catheterization and found some benefit from a 20-minute massage intervention.303 In the treatment group, systolic blood pressure was reduced a mean 8.6 mmHg and perceived psychological distress was reduced as well. The mechanism of benefit in massage therapy appears to be both a reduction of anxiety levels and an increase in cardiac parasympathetic activity. The MANTRA studies suggest clinical benefit on cardiac outcomes in patients undergoing angioplasty with therapeutic touch,but no significant difference was seen between treatment groups. Additional trials seem warranted, as is evidenced by the validity of massage therapy to reduce stress, which is a major provocative factor in CAD.
Sep
7
2023
Fascial Unwinding: Tissue Memory (4)
A literature review from manual therapy books as well as scientific literatures was conducted to find possible explanations and theory on why and how unwinding occurs. This includes: tissue memory, fascia and myofascial release theory, neurobiological explanation, ideomotor action, and consciousness model.
Tissue memory
The metaphors used to explain fascial unwinding include: unwinding tangled telephone wires (Frymann, 1998) or unwinding twisted rubber bands (Brooksby, 2005). The most common explanation that can be found in manual therapy books is that tissues hold memory of trauma, and unwinding will allow the client’s body to move to self correction (Manheim and Lavett, 1989). Sills (2003) states that the motions are often expressions of frozen stress responses and unresolved trauma.
Upledger and Vredevoogd (1983) described it as follows:
“When an injuring force occurs, the tissue which receives the force changes. Perhaps it retains the energy of the impact. A level of increased kinetic activity or higher entropy is set up in the impaired area. The human body then either dissipates that energy and returns to normal; or the body somehow localizes the impact energy and walls it off.”
Upledger (1987) developed the concept of energy cyst as “a localized area of increased entropy, which the host’s body has walled off.” These energy cysts are areas in which kinetic energy is now stored as potential energy in the connective tissue matrix.
“Energy cysts are essentially considered to be regions of foreign energy that are disorganized and which do not allow the normal conduction of microelectric currents through these disorganized regions. The disorganized energies may be thought of as entropic. They usually seem to derive from non-physiologic sources, such as from external trauma, pathogenic organisms or severe emotional shocks, etc. The body appears to be unable to discharge these ‘foreign’ energies and as an alternative minimizes their effect by compressing them into the smallest possible volume.” (Upledger, 2000). Unwinding attempts to free these stored energy. (Upledger, 1987)
Another attempt to explain it incorporates a bit of physics terminology: “Unwinding is an exothermic process in which the kinetic energy originally imprinted in the tissue is released as heat” (Alexander, 1998). It is also added that when the unwinding is taking place, the client’s may re-experience thoughts and feelings that they had when the tissue was originally injured.
In bodywork literature it is generally accepted that fascia or connective tissues can hold memory and trauma (Upledger, 1987; Rosen and Brenner, 2003; Barnes, 2004; Paoletti, 2007). This tissue memory is believed to cause the unwinding phenomena. The idea of tissues can store memory independent of the nervous system is discussed in length by Chaitow (2003) and Oschman (2006).
There are various theories regarding memory for traumatic events maybe encoded differently from other events. The first is called state-dependent memory which comes from observation that memory in one state of consciousness cannot be recalled until the person returns to the same state. Another idea is suggested by Freud, who proposed that unwanted memories can be excluded from awareness, a process called repression. Anderson et al. (2004) showed that a biological mechanism exists in the human brain to block unwanted memories. Using functional magnetic resonance imaging Anderson et al. (2004) identified the neural systems involved in keeping unwanted memories out of awareness. Depue et al. (2007) showed further evidence including neural mechanisms. This idea also means that the neurobiological mechanism can be recruited to control memory retrieval as well.
Barnes (1990, 2000) suggested position-dependent memory, learning, and behavior. Trauma or memory can be state or position dependent and can be retrieved when the client is in a particular state or position. Unwinding is said to assist in bringing the repressed memory to a conscious level, allowing clients to re-experience it and let go.
Although a specific touch or body positioning can trigger specific memory associated with it, yet it cannot be proven that that particular memory is stored in those tissues or cells. Scientific evidences regard this as “triggers” for a memory, while the memory is still “stored” within the central nervous system.
Sep
7
2023
Spontaneous Bodywork
Here’s some videos of therapeutic techniques that use the body’s own spontaneous movement
Myofascial Unwinding
Simple Contact
Created by Barrett Dorko PT, which used the reflexive reaction of the body to gentle touch at specific sites. It begins with the premise that the body’s own corrective processes are generally sufficient to produce enough mechanical force to reduce pain and normalize function.
Muscle Repositioning
Founded by Fernando Bertolucci, a physician and Rolfer from San Paolo, Brazil. It is a type of myofascial release characterized by integrating body segments. Spontaneous movements can occur during the treatment.
Facilitated and spontaneous movement
A variation of the indirect osteopathic technique
