Sep
8
2023
Unwinding as an ideomotor action
Barret Dorko (2003) suggested that fascial unwinding can be explained as ideomotor movement (ideomotion). He postulated that cranial techniques founded by Sutherland and palpated inherent tissue movement fall into this category. As stated by Ward (2002):
“Inherent tissue motions are palpably evident, asymmetrically patterned, neuroreflexive activities in the soft tissues. They constantly move, often at variable rates. Palpation that focuses on these motions should readily identify patterns of shifting asymmetric tightness and looseness.”
Ideomotor action or ideomotion is “influence of suggestion in modifying and directing muscular movement, independently of volition”, a definition given by psychologist/physiologist William Carpenter in 1852.
Carpenter used ideomotor action as an explanation for various phenomena that were being credited to new physical forces, spiritual intervention, or other supernatural causes (Hyman, 1999). Later, William James in 1890 proposed a wider meaning that ideomotor activity is the basic process underlying all volitional behavior:
Ideomotor action also pertains to body movements that can arise in observers watching other people perform certain actions (Knuf et al., 2001). Muscles can be involuntarily activated by thoughts. Involuntary muscle movement can manifest in various ways, for example asking a subject to think of an activity is enough to set the muscles required for that activity into action (Spitz, 1997).
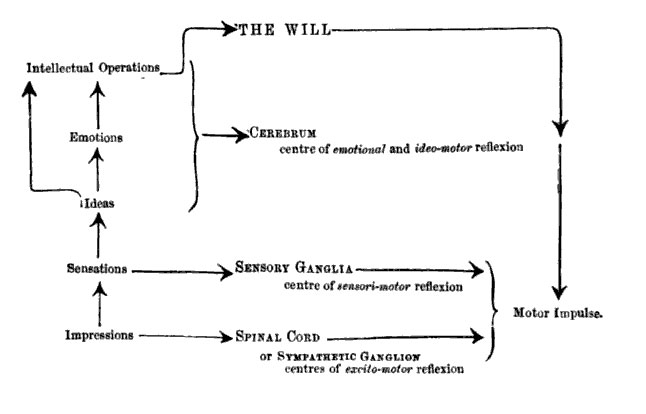
Carpenter (1860) characterized ideomotor action as a third law of reflex. Apparently at that time reflex movements are partitioned into two kinds: excito-motor (such as breathing and swallowing), and sensory-motor (such as surprise-reactions to a loud noise). Carpenter imagined the processing of stimuli and the generation of action as a bottom-up path of information processing. In the normal course of processing external impressions evoke sensations, ideas, emotions, and intellectual processes that determine the will. Then the will initiates the actions to be executed. But if the path of processing is interrupted at any point, Carpenter suggested that a reflex action occurs (Stock and Stock, 2004).
On the lower levels there are excito-motor reflexes, which are controlled by the spinal cord. On the next highest level of processing sensory-motor reflexes set in, controlled by the sensory ganglia. Finally, the ideo-motor reflexes occur, when the will, as the highest controller, is turned off in some way. In this case ideas and emotions gain direct access to action execution through reflexes (Figure 1, Carpenter, 1860).
Dorko (2003) hypothesized the mechanism of unwinding as follows: “Muscular pain can arise from mechanical deformation of various tissues. If the movement required for reducing that injury is not permitted because of cultural norms, the body would respond with an array of isometric contraction of muscular activity.”
Dorko further hypothesized that this muscle activity is commonly misinterpreted as a lack of appropriate relaxation, and subjected to various forms of stretching, manipulation or exercise. Unwinding allows full expression of the muscles and encourages completing the motor response for which the contraction was activated. The touch by the therapist is gentle and non-coercive, with a goal to make the client aware of internal motor activity and then get out of the way of that movement.
This seems to be in accordance with the Rosen method (Rosen and Brenner, 2003) which believes that our bodies and characters are shaped by the social factors, developing habitual patterns of holding and restriction in order to be socially appropriate. Our muscles were tightened to inhibit the expression of emotions and physical motions of defense. These inhibited emotions and motions are stored in the body limiting our freedom of expression and movement.
McCarthy et al. (2007) suggested that the resolution of muscular pain is dependent on an appropriate motor response, and such a response should proceed as the result of instinctive, in-built mechanisms. Ideomotor movements constitute the prevailing expression of instinctive movement response. They hypothesized that the corrective ideomotor movement expression may lead to improvements in pain intensity and disability in symptomatic clients whose instinctive responses have been suppressed.
